Best Exercises for Serratus Anterior, Levator Scapulae and Rhomboids (Part 2)
Selecting the right exercises for the serratus anterior, levator scapulae, and rhomboids is key to improving shoulder stability and reducing pain. This article breaks down the best evidence-based movements to strengthen these muscles effectively.
September 15, 2015
3 min. read
This is Part 2 of the Evidence-Based Strength Training Series. In the first article, we looked at the often-neglected scapulothoracic muscles, their functions and the best exercises to recruit them.
In the article:
Scapulothoracic Muscles and Pain
As I mentioned in Part 1, weakness or poor neuromuscular control of the periscapular muscles has been implicated in subacromial impingement1,2, lateral epicondylalgia3-5, cervicogenic headache6, and neck pain7,8.
Specifically, insidious onset of neck pain and whiplash-associated disorder (WAD) have been linked with a significant delay in and shorter duration of serratus anterior activity bilaterally during arm elevation9. A similar study found decreased serrates anterior activation in individuals with acromioclavicular osteoarthritis and rotator cuff disease.10
Although a cause-and-effect relationship cannot be confirmed, this preliminary evidence still lends support for targeting the periscapular muscles in individuals with neck or shoulder pain.
EMG Activity and Exercise Goals
According to Reiman et al.11 and Escamilla et al.12, moderate EMG activation (21-40% MVIC) is best used to facilitate endurance and neuromuscular re-education; high activation (41-60+% MVIC) promotes strength gains.
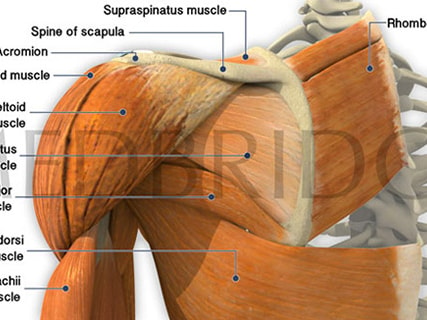
From Biomechanics to Exercises
Serratus Anterior
Primary Function: scapular upward rotation, external rotation, posterior tilt at the acromioclavicular joint, protraction of the clavicle at the sternoclavicular joint.
Origin: External surfaces of lateral aspect of 1st-8th ribs
Insertion: Anterior surface of medial border of scapula
The SA is often activated with scapular protraction. The exercises yielding the highest MVIC for the serratus anterior include:
dynamic hug13
push-up plus13
scaption with external rotation14
diagonal PNF (shoulder flexion, horizontal flexion, external rotation)15
shoulder abduction in scapular plane above 120 degrees15
The upper trapezius (UT) often compensates for a weak or inhibited serratus anterior, so its beneficial to selectively activate the SA in lieu of the UT. According to Cools and colleagues, the best SA:UT ratio is achieved in:
high row
forward shoulder flexion
scaption with external rotation14


| [Table] MVIC values for SA exercises |
Levator Scapulae
Primary Functions: scapular elevation, glenoid cavity inferior tilt through upward scapular rotation
Origin: Posterior tubercles of transverse processes of C1-C4 vertebrae
Insertion: Medial border of scapula superior to root of scapular spine
These muscles have received little attention in the literature compared the SA or trapezius. In a study, Moseley and colleagues discovered that the levator scapulae achieves the highest activity in:
rowing
horizontal abduction
shrug
horizontal abduction with ER
prone shoulder extension16
| [Table] MVIC values for Levator Scapulae exercises |
Rhomboids
Primary Functions: Retraction of the scapula; upward rotation to depress glenoid cavity; scapular attachment to thoracic wall
Origin: nuchal ligament; spinous processes of C7, T1 and T2-T5 vertebrae
Insertion: smooth triangular area at medial end of scapular spine; medial border of scapula from level of spine to inferior angle
The rhomboids achieve the highest MVIC during:

| [Table] MVIC values for rhomboid muscle exercises |

Choosing the Best Exercise
These studies give us a glimpse into properly selecting exercises, yet very few exercises have been or will ever be studied.
When choosing an exercise for your patient, be sure to consider:
the biomechanics of the movement,
current evidence for or against the exercise,
your patient's presentation and goals for treatment.
aggravating movement(s) or comparable signs
For more information on treating shoulder dysfunction, check out Eric Hegedus's course Evidence-Based Treatment of the Shoulder: An Update.
Below, watch a video from the Medbridge's Patient Education library explaining rotator cuff tears.
Meet the Author


Subscribe to Our Newsletter
Related Posts

June 21, 2016
Best Exercises for the Trapezius Muscle
By John Snyder

September 11, 2018
9 Best Scapular Exercises to Perform for Shoulder Impingement (and 4 Alternates)
By Jennifer T. Dodson

November 21, 2019
From Dancing to Dunking: Rotations of the Scapula
By Aaron Sciascia

January 12, 2023
Defining Scapular Dyskinesis and Its Causes
By Aaron Sciascia